Knee joint is a complex and largest joint in our body. This modified hinge joint consists of two main components: 1) The ‘tibio femoral joint’ (where tibia meets femur) 2) The ‘patello femoral joint’ (where the knee cap meets the femur).
Forces equal to 3 times of one’s body weight are transmitted through the knee during normal walking, which further increase to about 8 times our body weight during squatting. These enormous amount of pressure passing through the knee joint makes it vulnerable to injury while providing flexion (bending) movement.
Bones of the Knee
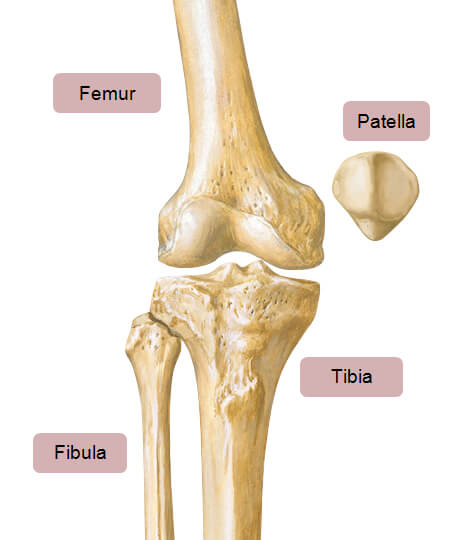
There are 4 bones around the knee namely: Femur (thigh bone), Tibia (shin bone), Patella (knee cap) and Fibula.
![[Click here for High Resolution]](http://thekneeworld.com/wp-content/uploads/knee/anatomy-bones-of-the-knee.jpg){kind=link}
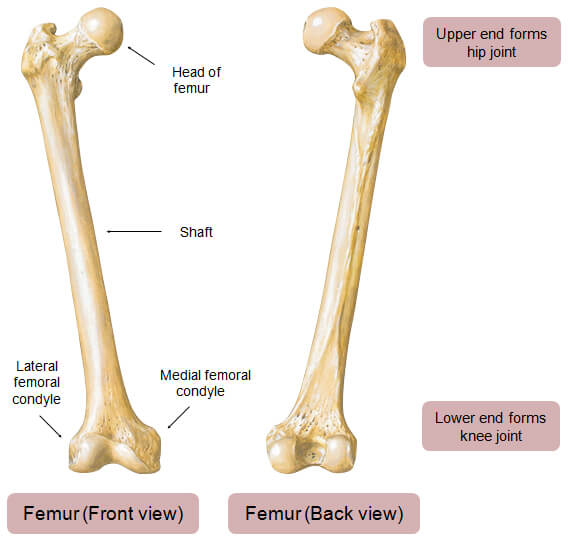
Femur (thigh bone)
It is the longest bone in the body. Lower end of femur forms broad round structure called as ‘femoral condyle’, two in number, medial (inner) and lateral (outer). Within the knee joint, the end of the femur is covered with cartilage which articulates (unites) with the upper ends of tibia (shin bone) to form ‘Tibio femoral joint’.
![[Click here for High Resolution]](http://thekneeworld.com/wp-content/uploads/knee/anatomy-femur.jpg){kind=link}
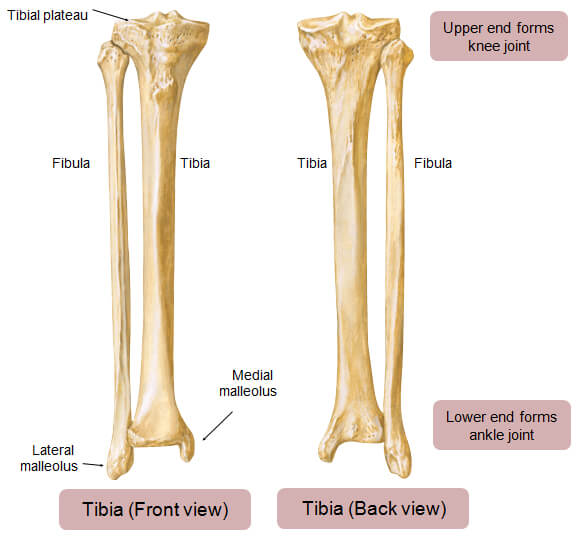
Tibia (shin bone)
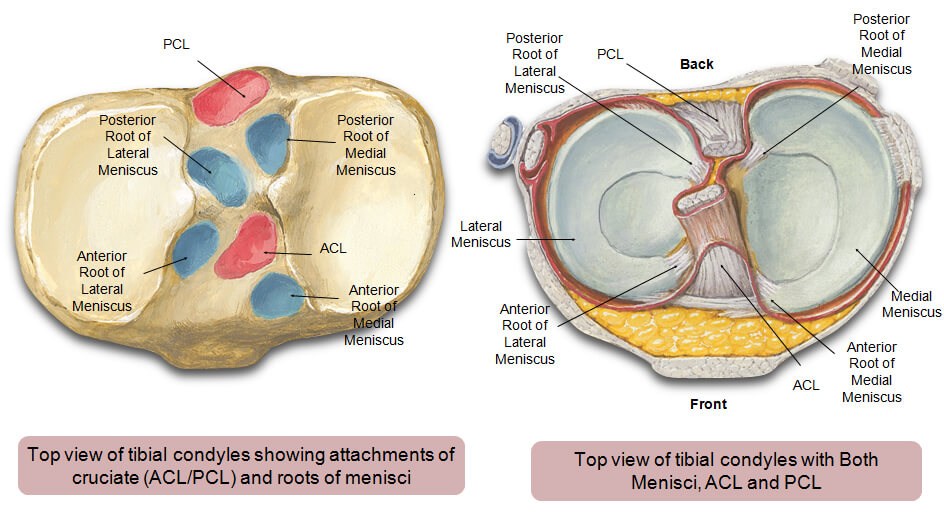
It extends from knee to the ankle. Upper end of tibia forms broad oval shaped platforms called ‘tibial plateaus’ which are covered with cartilage to articulate with femoral condyles. Additionally, upper surface of the tibial plateau provides attachment for two C-shaped shock absorbing cartilages called ‘menisci’.
![[Click here for High Resolution]](http://thekneeworld.com/wp-content/uploads/knee/anatomy-tibia.jpg){kind=link}
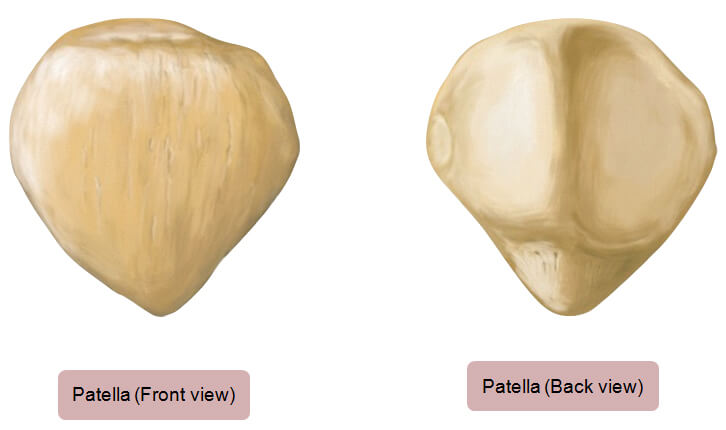
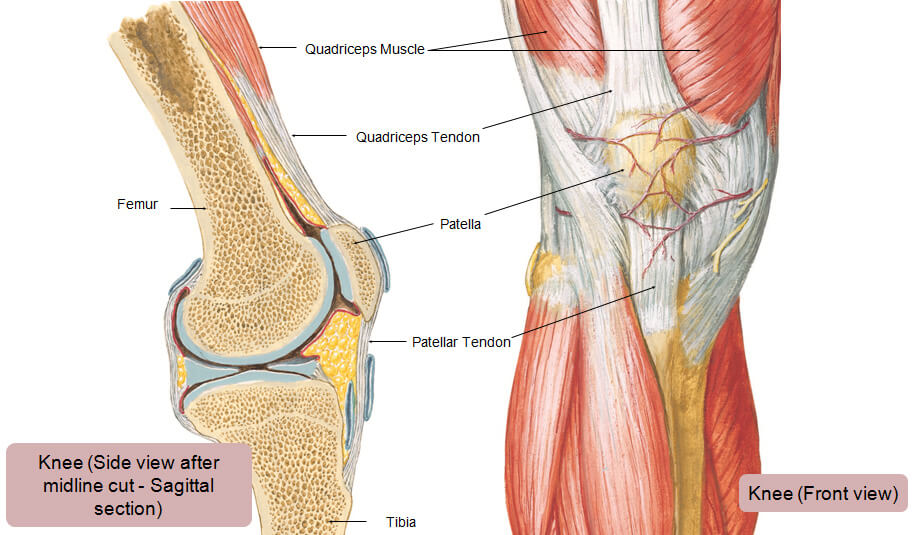
Patella (knee cap)
It is a triangular, semi-flat bone on the front of the knee. Patella provides attachment to the quadriceps tendon on the top and patellar tendon at the bottom together creating a ‘quadriceps mechanism’. Patella acts as an important fulcrum for the extension (straightening) of knee through quadriceps mechanism, thereby increasing the force generated by quadriceps muscles. The back surface of the patella articulates with femur to form ‘Patello-femoral joint’.
![[Click here for High Resolution]](http://thekneeworld.com/wp-content/uploads/knee/anatomy-patella.jpg){kind=link}
Fibula
It is a thin long bone that runs adjacent to the tibia from the knee to the ankle. It contributes to the knee stability by providing attachment to muscles like biceps femoris and ligaments like fibular collateral ligament on outer aspect of the knee.
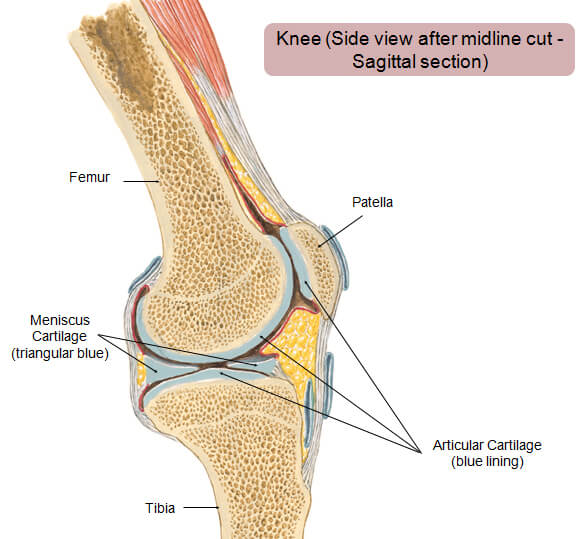
Articular Cartilage
Articular cartilage (also known as hyaline cartilage) covers the lower end of femoral condyles (thigh bone), upper end of tibial condyles (shin bone) and under surface of the patella (knee cap) to allow painless, smooth and low friction movements of knee joint. Joint fluid lubricates the articular cartilage and makes it even more slippery for smooth movements of the two bones. Wear and tear of cartilage leads to arthritis, which makes joint movements restricted and painful. Unfortunately, cartilage is avascular (without blood supply) and gets its nourishment from the surrounding synovial fluid (joint fluid). Thus, our body cannot repair a damaged articular cartilage effectively.
![[Click here for High Resolution]](http://thekneeworld.com/wp-content/uploads/knee/anatomy-articular-cartilage.jpg){kind=link}
Meniscus
These are 2 semi-circular cushion-like structures in between the lower end of femur (femoral condyles) and upper end of tibia (tibial condyles). Menisci are made offibrocartilage. It facilitates smooth movements during flexion and extension of knee. More importantly, meniscus allows effective load transmission across knee joint, improves joint stability, acts as a shock absorber and lubricates as well as nourishes the knee joint. Absence of menisci causes immense cartilage overload and risk of early wear leading to development of osteoarthritis. Therefore, injuries to menisci may need surgical treatment to retain their function.
![[Click here for High Resolution]](http://thekneeworld.com/wp-content/uploads/knee/anatomy-meniscus.jpg){kind=link}
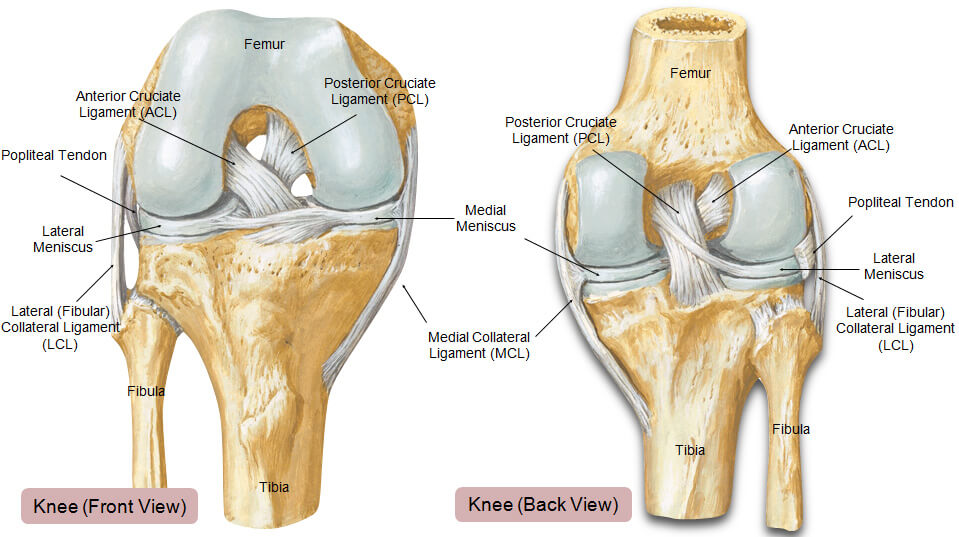
Ligaments of the Knee
Ligaments are soft tissues that connects one bone with another. They provide passive stability to knee joint. Also, they serve an important proprioceptive (joint sensation) function. The knee joint has two intra-articular (inside the joint) ligaments, ACL and PCL, which are oriented in criss-cross manner connecting tibia and femur. They provide mainly antero-posterior (front-back) stability to the knee joint. While the extra-articular (outside the joint) ligament complexes on medial (inner) as wells as lateral (outer) aspect of knee joint provide mediolateral (sideways) stability and rotational stability.
![[Click here for High Resolution]](http://thekneeworld.com/wp-content/uploads/knee/anatomy-ligaments-of-the-knee.jpg){kind=link}
ACL
‘Anterior Cruciate Ligament’ (ACL) is one of the two criss-cross ligaments present within the knee joint. It is primary anterior stabiliser and limits forward motion of tibia relative to femur. It is the most common knee ligament injured in pivoting sports and activities that involve sudden turning, stopping, jumping and landing. ACL tear, if left untreated, makes knee unstable which can lead to early arthritis.
PCL
‘Posterior Cruciate Ligament’ (PCL) is located in the back of the knee behind ACL. It is a primary posterior stabiliser and therefore limits backward motion of tibia relative to femur. Often PCL tear is associated with injury to other ligaments and meniscus.
MCL and PMC
On medial (inner) side of the knee, ‘Postero-medial complex’ (PMC) provides side-to-side stability resisting medial (valgus) opening of knee. Superficial medial collateral ligament (sMCL), deep medial collateral ligament (dMCL) and posterior oblique ligament (POL) are the most important components of PMC. MCL is a primary restrain for medial opening of knee, while POL is a primary restrain for internal rotation of tibia. Medial side of knee has another important stabiliser for patella known as ‘Medial patello-femoral ligament’ (MPFL). It plays important role in preventing patellar dislocation.
LCL and PLC
On lateral (outer) side of the knee, ‘Postero-lateral complex’ (PLC) provides side-to-side stability resisting lateral (varus) opening of knee. Three primary components of PLC are lateral collateral ligament (LCL), popliteus tendon (PT), and popliteofibular ligament(PFL). LCL, also known as fibular collateral ligament (FCL) is the primary restrain for lateral (varus) opening of knee joint, while PT and PFL provide primary external rotation stability to tibia. PLC injury is more commonly associated with injury to cruciates (ACL/PCL), meniscus or cartilage.
Joint Capsule
It is a thick, fibrous structure that wraps around the knee joint. Inside the capsule is the synovial membrane which is lined by the synovium, a soft tissue structure that secretes synovial fluid, the lubricant of the knee.
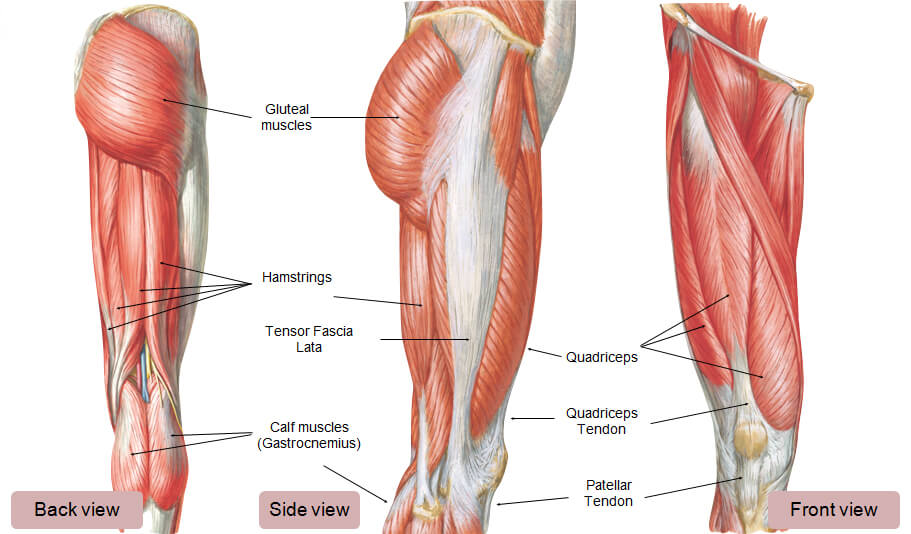
Muscles around knee joint
They help to keep the knee stable, well aligned and moving. There are two major group of muscles around knee- quadriceps and hamstrings.
Quadriceps are muscles on the front aspect of thigh. It is formed by 4 muscles namely rectus femoris, vastus medialis, vastus intermedius and vastus lateralis. They together form quadriceps tendon which is attached to the upper pole of the patella. Quadriceps is primary knee extensor responsible for straightening of knee from bent position.
Hamstrings are the muscles of the back of the thigh. It consists of 3 muscles – biceps femoris, semimembranosus and semitendinosus. Hamstrings help in bending (flexion) of the knee from straightened position.
Gluteal muscles (muscles of hip) provide additional stability to the knee joint and are crucial to the overall knee health.
![[Click here for High Resolution]](http://thekneeworld.com/wp-content/uploads/knee/anatomy-muscles-around-knee-joint.jpg){kind=link}
Extensor Mechanism of Knee
It comprises of quadriceps muscle group, quadriceps tendon, patella, retinaculum, patellar tendon and adjacent soft tissues. Integrity of extensor mechanism is crucial for effective extension of the knee. It increases the force generated by the quadriceps muscle needed to straighten the knee from bent position. Acute injuries, overuse injury or chronic degenerative injuries can affect the extensor mechanism and need timely management to preserve its function.
![[Click here for High Resolution]](http://thekneeworld.com/wp-content/uploads/knee/anatomy-extensor-mechanism-of-knee.jpg){kind=link}
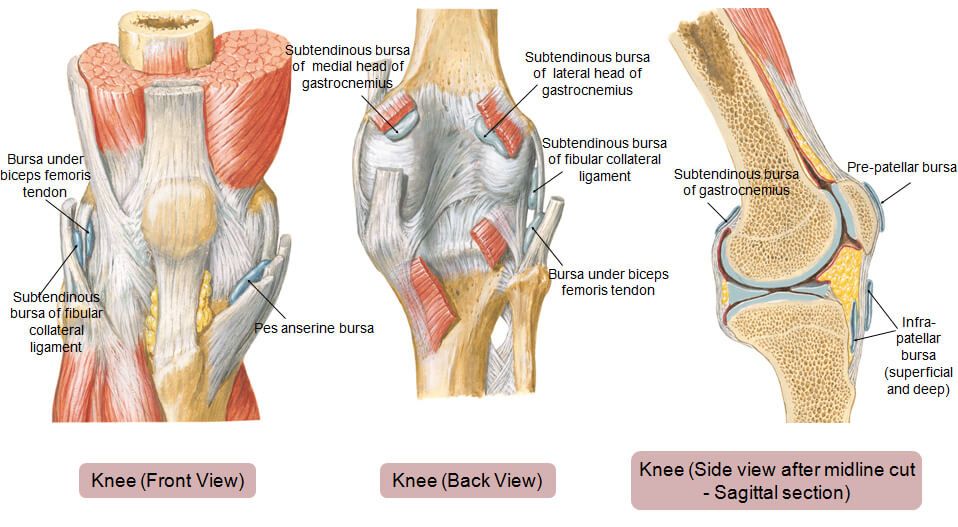
Bursae
There are up to 13 bursa of various sizes in and around the knee. These fluid filled sacs cushion the joint and reduce friction between muscles, bones, tendons and ligaments. There are bursa located underneath the tendons and ligaments on both the lateral and medial sides of the knee. The prepatellar bursa is one of the larger bursae of the knee and is located on the front of the patella (hence pre-patellar) just under the skin. It protects the patella. Sometimes, whether due to direct trauma or even infection, it can become irritated, swollen, and painful. This is known as prepatellar bursitis.
The pes bursa is another important bursa that overlies some of the hamstring tendons which attach to the medial side of the tibia. It too can sometimes become irritated, causing pes bursitis, which can be painful.
![[Click here for High Resolution]](http://thekneeworld.com/wp-content/uploads/knee/anatomy-bursae.jpg){kind=link}
Plicae
Plicae are folds in the synovium (inner lining of joint capsule) within the knee joint itself. Plicae rarely cause problems but sometimes can get caught between the femur and patella and cause pain.
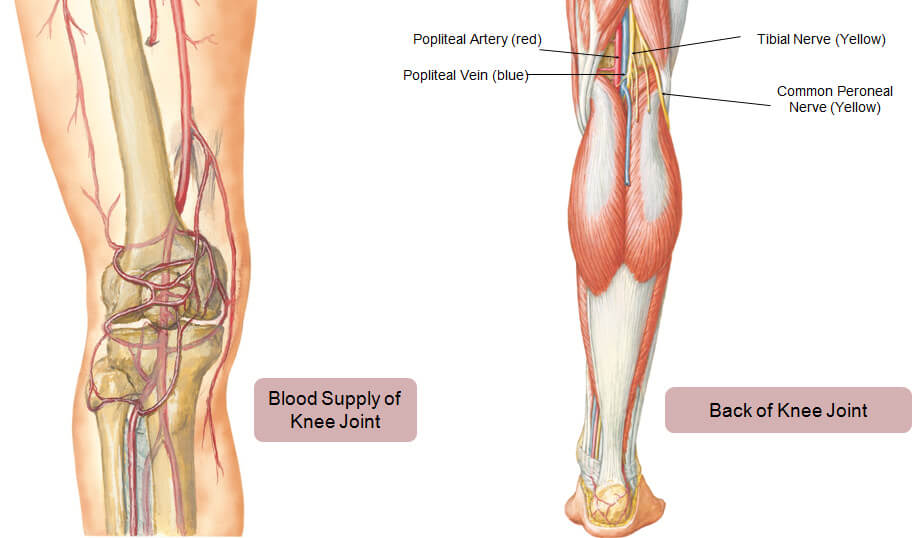
Knee Arteries and Veins
Probably the most important thing to know about the blood supply to the knee is that it is very abundant. There are many collateral vessels (basically extra vessels) that give blood supply to the structures of the knee.
Back side of the knee joint is in close proximity with the major blood vessels (popliteal artery and vein) and nerves (tibial nerve and common peroneal nerve) of lower limb, which puts them at risk of injury during fractures or surgeries.
![[Click here for High Resolution]](http://thekneeworld.com/wp-content/uploads/knee/anatomy-knee-arteries-and-veins.jpg){kind=link}